



Residents of B.C.’s largest cities are living longer than ever — but their counterparts in the B.C. Interior are not.
Twenty years of life expectancy data obtained by The Tyee reveals that the closer a community is to British Columbia’s largest cities, the longer its residents tend to live.
The data also shows that the life expectancy gap between B.C.’s most prosperous cities and its economically struggling areas is growing steadily larger.
In parts of Metro Vancouver, life expectancies are now approaching 90.
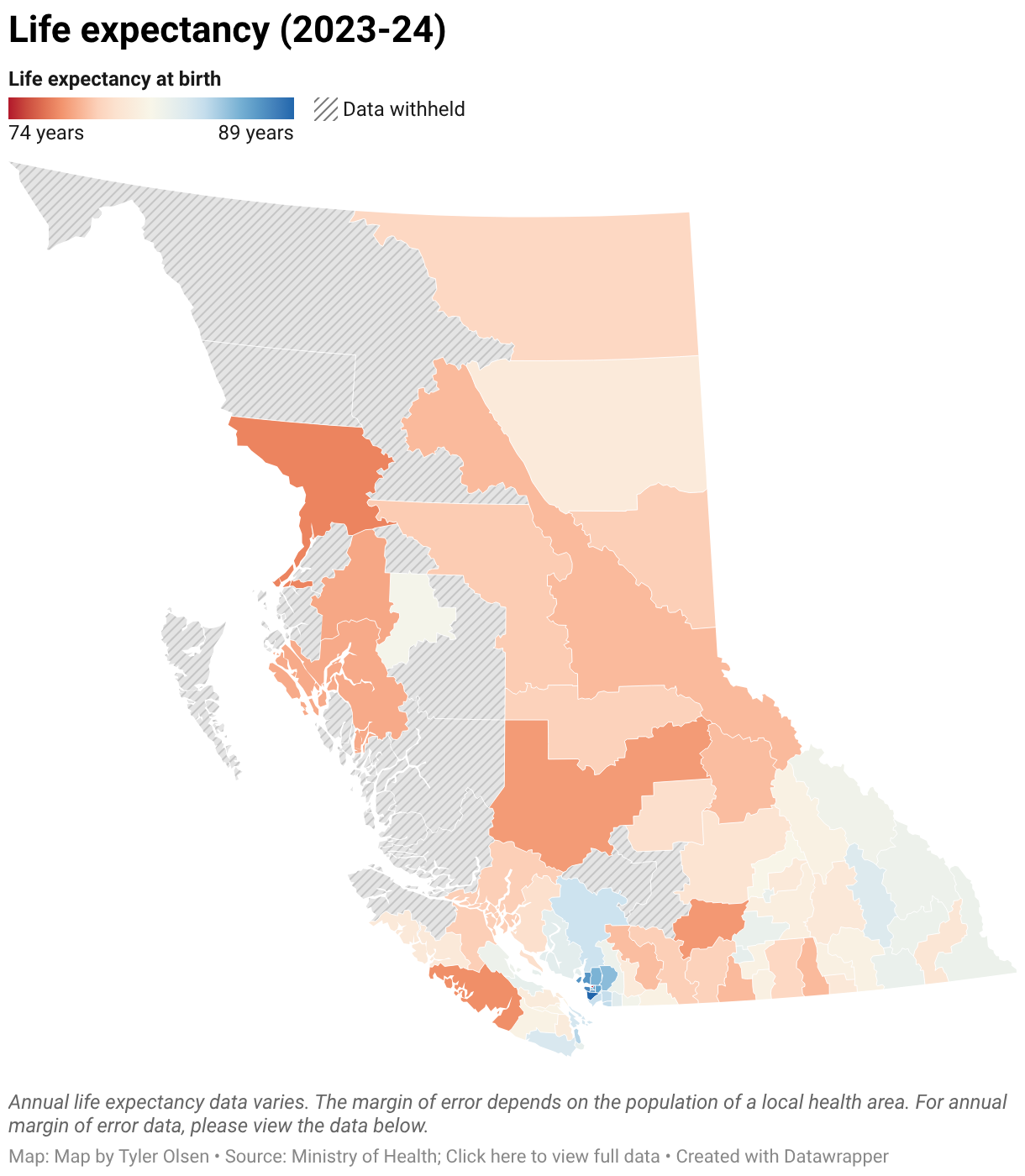
By contrast, in many Interior areas and the central Vancouver area surrounding the Downtown Eastside, projected lifespans have declined over the last two decades according to the figures, which were released to The Tyee by request but are not otherwise publicly available. The data reveals life expectancy, in jurisdictions called local health areas, between 2000 and 2024.
Richmond has British Columbia’s longest life expectancy, with residents born in 2024 expected to live 89.4 years on average. The second part of this Tyee series will examine why people in Richmond may live particularly long.
By contrast, the small but densely populated central area surrounding Vancouver’s Downtown Eastside has the province’s lowest life expectancy.
Life expectancy data reveals “a really important variable in public health for us to gauge how a community is doing,” Fraser Health medical health officer Dr. Curtis May told The Tyee.
Understanding those factors can inform health officials about challenges, and inform potential responses, May said.
Access to health care is important, but one of many components. Income, education levels, housing quality, interactions with toxic drugs, and other external factors all play key roles in determining the life expectancy of broad and diverse populations. Environmental and social factors and the prevalence of healthy or risky habits also affect a community’s overall health, and the length of the lives of its residents.
“This is a whole-of-society story,” May said.
The longest, and shortest, lives
Across British Columbia, the life expectancy at birth in 2024 was 82.6 years, according to the most recent data from Statistics Canada.
That’s higher than in 2004, when babies could be expected to live for 80 years, on average.
But the two decades of provincial life expectancy data provided to The Tyee show just how varied life expectancies are across the province. The data, which stretches from 2000 to 2024, shows significant progress in some local health areas, but decreases in other places.
The areas themselves vary significantly in size and population in ways that could affect the data. Vancouver is broken into six local health areas, while Surrey — which has a similar population — is divided into two areas. Most large B.C. municipalities are covered by a single local health area. Local health areas in less-urban regions often include multiple communities.
In addition to Richmond, eight other local health areas have life expectancies exceeding 85. All are in the Lower Mainland, and four are within Vancouver. The other long-lived areas include North Vancouver, West Vancouver, Burnaby and the Tri-Cities — which encompasses Coquitlam, Port Coquitlam and Port Moody, and the two villages of Anmore and Belcarra.
Life expectancies in Victoria and the Kelowna area have also continued to tick upwards, with babies in the Greater Victoria area expected to live about 83 or 84 years, and with life expectancies in the Kelowna area about 82 years and in line with the provincial average.
With a few exceptions in the Kootenays and the Comox area, life expectancy recedes as one travels away from B.C.’s largest cities. In the Fraser Valley, for instance, people in Surrey are expected to live longer than those in Langley, who have longer projected lives than neighbours in Abbotsford, who live longer than those in Chilliwack. By the time one gets to Hope and Agassiz-Harrison, barely an hour outside of Vancouver, life expectancies dip below 78.
Communities farther inland have even lower life expectancies. Merritt, just up the Coquihalla, had a life expectancy of 76.6 in 2024. On Vancouver Island, the life expectancy in Alberni-Clayoquot and Greater Campbell River is well below that of communities to their east and south.
The life expectancy data provided by the ministry are statistical estimates with margins of error that vary depending on the size of each health area’s population. By tracking the figures across multiple years, the data becomes more precise and reveals clear health trends.
Progress, and regression
The life expectancy gap between wealthy urban areas and less-wealthy and more-rural areas has increased significantly over the last two decades, the data shows.
At the turn of the millennium, life expectancies in Metro Vancouver ranged from 80 to 83 years outside of the Vancouver-Centre North local health area that includes the Downtown Eastside.
To the east, in Fraser Valley communities such as Hope and Chilliwack, and in the Interior, life expectancies were only two or three years shorter. Life expectancies in the Interior were broadly similar.
But over the last two decades, life expectancies in relatively wealthy urban and suburban areas around Vancouver and Victoria have steadily advanced, and those in the Interior have generally stalled or retreated.

In Richmond, life expectancy rose from 83 in 2001 to 89 last year. In the Squamish area and the western suburbs of Victoria, life expectancy increased from 80 to 84. That pattern exists across the Lower Mainland except for the area around the Downtown Eastside.
In that area, the data paints a tragic picture of aborted progress. There, life expectancy rose significantly between 2001 and 2014, increasing from 73 to 80 years. But that progress began to reverse itself as the toxic drug crisis worsened. By 2024, all the previous gains had been lost. The arrival of COVID in the spring of 2020 delivered an additional hit to life expectancy in the area.
A less extreme version of that story is mirrored across the province, particularly in many smaller, more-rural local health areas.
All over the Interior of the province, life expectancy rose from the high 70s in 2000 to the low 80s by 2014, only to retreat over the following decade.
By 2024, life expectancy across much of B.C. was lower than it had been 10 years earlier. Over that decade, it declined by more than one per cent in 26 local health areas and increased by more than one per cent in 18 areas. Of those places recording increases, 13 were in the Lower Mainland. Of the 26 areas with decreased life expectancy, 18 were in the Interior Health or Northern Health authority regions.

The pattern of rising, then falling life expectancy repeated itself in Cranbrook, Kamloops, Grand Forks, 100 Mile House, Penticton and many other communities.
The Cariboo-Chilcotin — the local health area including and surrounding Williams Lake — saw one of the most significant drops in recent years. In that region, life expectancy rose from 78 around 2001 to 80 around 2014. But over the following decade, life expectancy plunged to 76. The third story in this series will look at the challenges particular to that region of B.C.
The challenges
The province redacted data for several rural areas with small populations and large Indigenous populations. A Ministry of Health official wrote that information that could reflect Indigenous health outcomes requires the ministry “to uphold Indigenous data governance principles” and engagement with Indigenous communities.
The unredacted provincial figures echo a 2024 report on life expectancy among B.C.’s Indigenous people. That report by the First Nations Health Authority and the Office of the Provincial Health Officer showed the life expectancy of First Nations people in B.C. plunged from 73 in 2017 to 67 in 2021. The decline further widened the gap between the projected lifespans of Indigenous and non-Indigenous residents.
“This life expectancy data is gut-wrenching,” Dr. Danièle Behn Smith, the province’s deputy provincial health officer for Indigenous health, told media at the time.
First Nations Health Authority chief medical officer Dr. Nel Wieman said at the time that the report underscored “persistent gaps in B.C.’s health and supportive systems which continue to fall short of their responsibilities to First Nations Peoples in B.C., their families, communities and Nations.”
Although the Ministry of Health redacted data for some areas with very high concentrations of Indigenous patients, many regions where life expectancy has declined also have significant First Nations populations.
When asked about the challenges faced by First Nations, Interior Health medical health officer Andy Delli Pizzi highlighted the 2024 report.
“So many communities and nations are flourishing, and yet there remains this discrepancy,” he said. Delli Pizzi noted that the 2015 Truth and Reconciliation Commission of Canada final report called on both Canadians and government to acknowledge that the gap in health outcomes was the result of historic and ongoing colonial policies.
“Unfortunately, the gap has widened since then,” he said.
The discrepancy is painfully obvious to Łučinłc̓uta, the chair of the First Nations Health Council and a member of the Hesquiaht First Nation near Clayoquot Sound. Łučinłc̓uta, who also uses the name Mariah Charleson, told The Tyee that she recently attended five funerals in a single month. None of the people who had died had made it to the age most Canadians can expect to live. The funerals are now depressingly common, Łučinłc̓uta said, and the significantly lower life expectancy of First Nations people “should ring alarm bells.”
Łučinłc̓uta said the challenges expose the lingering damage of residential schools and the need to empower First Nations, increase health-care funding for Indigenous communities and address the “layers upon layers of colonization” that affect people’s lives and well-being.
“Resources are a big part of it but it’s not the [only] answer,” she said. “There’s so much layers of well-being — the physical, spiritual, emotional — it can’t all be solved with just money and resources. It’s much deeper than that.”
Addressing those deeper challenges requires allowing First Nations peoples to revitalize their languages, cultural practices and relationships to their traditional territories, she said.
Asked about what it had done to address the continued gap in health outcomes, B.C.’s Health Ministry cited improvements to its travel assistance program for people in First Nations and remote communities; the hiring of more Indigenous health navigators to advocate for Indigenous people; the creation of primary care networks in remote areas; and increased Indigenous representation on health boards and committees.
The building blocks of health
Some of the life expectancy figures provided by the province may be influenced by the geographic boundaries of local health areas.
Outside of Vancouver, local health areas include both impoverished areas and wealthier neighbourhoods in most communities. But because Vancouver has so many different local health areas, the Vancouver data highlights the gaps between individual neighbourhoods that, in other communities, would be included in a single number. In Metro Vancouver, the data can also highlight service disparities between communities and areas; Richmond’s high life expectancy may be partly the result of at-risk people choosing to live in communities with more service delivery organizations and facilities such as overdose prevention sites.
Despite the data’s potential shortcomings, the figures are still useful to health officials.
Life expectancy “helps us understand the health and well-being of a population,” Delli Pizzi told The Tyee.
Delli Pizzi pointed to what he called the “building blocks of health” — the variety of social, economic and environmental conditions that determine the well-being of a community.
Factors such as income and the prevalence of toxic drugs have direct and obvious impacts on a community’s health. Other variables, such as education, can be less immediately clear but still play an important role. Many factors are linked to one another, but also exert their own direct force. Understanding how they affect people’s lives can prompt the creation of programs and supports to address their impact.
Education is one example.
“If you have higher education, you probably can get a higher-paying job,” May said. That translates to income levels and access to healthy food, recreation opportunities, mental health supports and other elements of a healthy life. But education itself can increase one’s odds of living longer.
“If you have a higher education, you are more literate, especially in health, so you understand what the health system is telling you, what your doctor is telling you, and you can choose healthier options.”
Education is also linked to employment opportunities and the toxic drug crisis; men working in the trades are overrepresented among those who have suffered fatal overdoses, a key influence on life expectancy data.

Proximity to health care, access to transportation
Paul Adams, the executive director of the BC Rural Health Network, said geography itself also plays a major role in community health.
Transportation barriers and the distance to health-care services provide unique and real obstacles for people living in rural areas, Adams said.
“Rurality, just geography alone and the lack of transportation, becomes a huge driver” of poor health, said Adams, a Princeton resident who has Parkinson’s disease. Before he was diagnosed, Adams had about 20 procedures done, he said. Those required considerable travel and had to be booked individually. For some people, that presents a major barrier.
“There's no co-ordination happening on behalf of the patient; the onus is on the patient,” he said. “The patient may have mental health challenges and a variety of other issues to deal with, and whether they're capable of actually co-ordinating and advocating for their own co-ordination of care is questionable most of the time.”
Other cultural and social challenges also exist, including a lack of understanding that Adams said he observes between city-based health authorities and people in rural areas. Media consumption habits and the decline of local journalism have aggravated these disconnects, he said.
“Most of the information rural communities are now receiving doesn’t come from local media outlets,” he said. Adams said the focus of large outlets on major cities and a decline of local media outlets often prompts residents of rural areas to fill their news deficit by consuming information from platforms such as Facebook, and sources that tout unscientific information about health issues such as COVID and vaccination. Governments and health officials, he said, have not figured out how to counter that.
“Government information often comes from a top-down perspective,” he said. “In rural communities, you have to reach them where they're at, at the grassroots level. You have to find champions within community that are going to bring that information to them from the bottom up, and that has been a very difficult thing for government to get its head around.”
Challenges in First Nations communities
Despite struggles, the data released by the province suggests there is some hope.
The final year of data, 2023-24, shows an uptick in life expectancy in many B.C. regions that had previously seen declines. It’s unclear if that has continued — federal data for more recent years hasn’t yet been released — but the increase coincides with easing reduced rates of fatalities associated with toxic drugs and COVID.
The hope is that as those external factors recede, positive forces begin to reassert themselves.
That can include both population health programs meant to address the struggles of some regions, and the natural assets of the communities themselves. In countrywide surveys, residents of rural areas often report feeling more connected to their local community, Delli Pizzi noted. They often also have access to recreational and natural environments that contribute positively to health.
May, meanwhile, stressed that addressing the factors that shorten lifespans can also lead to better, happier lives.
“It’s not just about longevity,” he said. “It’s also about quality.”
This story is the first in a series about how life expectancy varies across BC. On Thursday, The Tyee will publish a piece taking a more in-depth look at why life expectancy in the Cariboo-Chilcotin is significantly lower than the provincial average — and why it has declined since 2014.

Read more: Indigenous, Health











Tyee Commenting Guidelines
Please note that email notifications for replies are not currently working due to a software issue which may be resolved in a future update.
Comments that violate guidelines risk being deleted, and violations may result in a temporary or permanent user ban. Maintain the spirit of good conversation to stay in the discussion and be patient with moderators. Comments are reviewed regularly but not in real time.
Do:
Do not: